Implementing A Mental Health Programme
Document
type: Micro-report
Author:
Christina Butterworth RN, SCPHN, Hon.FFOM
Publication
Date: 19/09/2017
-
Read the full document
1.0 Introduction
Organisations want a workforce that is fit to do the work they are employed to do and are aware that individual health status fluctuates over time, requiring understanding and support to minimise the negative effects and maximise the positive effects.
Crossrail incorporated its mental health programme into its overarching occupational health and wellbeing strategy, partly to normalise the promotion of good mental health and in recognition that you cannot have good physical health without good mental health.
2.0 Background
There is good evidence that work is good for people’s mental and physical health and wellbeing and that common mental health conditions are common within the general population and the working population. With mental health
 conditions (stress, depression and anxiety) accounting for 37% of all new and long-standing cases of work related ill health[1].
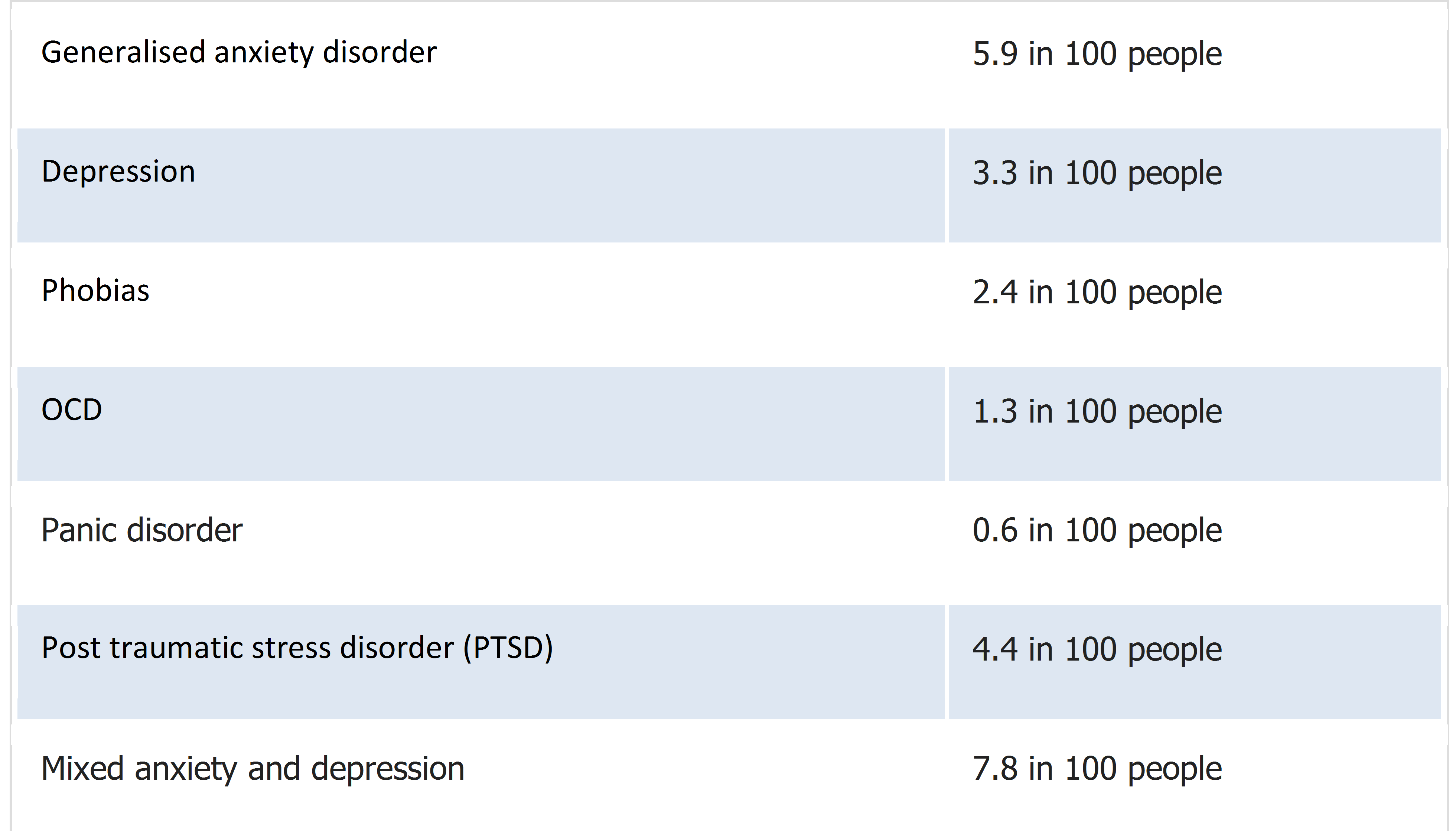
conditions (stress, depression and anxiety) accounting for 37% of all new and long-standing cases of work related ill health[1].Though the overall number of people with mental health conditions has not changed significantly in recent years, with approximately 1 in 4 people in the UK experiencing a mental health problem each year, how people cope is getting worse in terms of self harm and suicide. Table 1 outlines the issues as identified by the mental health organisation MIND:
Table 1 – Mental health Conditions
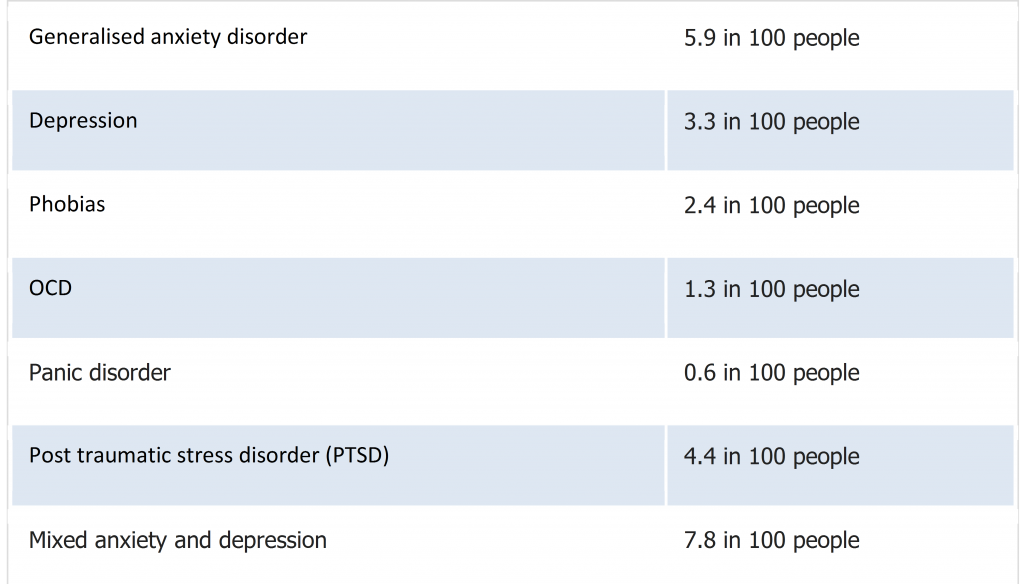
[Source: https://www.mind.org.uk/information-support/types-of-mental-health-problems/statistics-and-facts-about-mental-health/]
Statistics published by the Office for National Statistics in 2017[2] showed that men aged between 20 and 65 working in the construction industry between 2011 and 2015 had the highest rate of suicide in England, compared to other occupation groups.
3.0 Business Case
A business case was presented to senior management that was aimed at raising understanding about the prevalence of mental ill health at work, its impact on performance and the potential effectiveness of a range of interventions.
Defining mental health was important to demonstrate the wide spectrum of conditions from everyday pressures, worry and grief, to common mental health conditions such as anxiety and depression and even psychosis. Too often mental health is automatically associated with psychosis or stigma related to weakness or fear, when it is usually the ups and downs of life and common mental health conditions that are most prevalent and which can be managed more readily.
Definition: Mental health is a state of well being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully and is able to make a contribution to his or her own community.
(World Health Organisation)
Research by the Centre for Mental Health in 2009[3], estimated that the cost of mental health problems to business was over £1,000 per employee per year. This took into account lost working days through sickness absence, reduced productivity by employees underperforming at work (also known as ‘presenteeism’), and the cost of replacing staff who leave their jobs due to mental ill-health.
Mental health is personal to every individual, so the mental health programme needed to provide a blended approach that included; general awareness of mental health conditions, resilience and how to support self and colleagues.
The final case for change was a moral one that challenged senior managers to support the introduction of a mental health programme. The premise identified was ‘People are our greatest asset and we need to provide the resources required to manage their mental health and wellbeing.’
4.0 What did Crossrail Do?
4.1 Review and Plan
A review of the literature, good practice and resources was conducted and the ACAS and Mindful Employers training pack[4] was identified and used as the basis for the Crossrail mental health and wellbeing programme.
The timing of the review coincided with; an increase in media coverage on mental health issues, the launch of the Construction Industry Leadership Group workstream on mental health [5], the Public Health Responsibility Deal[6] and the London Healthy Workplace Charter[7], which each included a section on mental health. Further research was also being conducted by a number of mental health charities. All of which provided the visibility needed to support the implementation of the mental health programme and added weight to the business case.
Three themes were highlighted on which to base the programme:
- Tackling the stigma around mental health
- Focusing on the practical things that can be done to help
- Develop solutions by listening
4.2 Intervention
In addition to being based around the three identified themes the mental health programme was built on the three levels of health intervention:
4.2.1 Primary Intervention
Primary interventions focus on preventing poor mental health and wellbeing, through effective leadership practice.
This required executive commitment to key elements. These were identified as: a mental health and wellbeing survey (required to understand the mental health needs for the organisation); the performance review process needed to demonstrate return on investment; specialist advice and support needed to be integrated in the Crossrail management system. The contractual requirements of the Principal Contractors also needed to reflect what was required.
4.2.2 Secondary Intervention
Secondary interventions focus on reducing the impact of poor mental health and wellbeing, through screening, training/education and encouraging early personal strategies.
Focus was placed on awareness training for line managers to support the workforce; specific training for high risk groups; life-skills training for individuals, and a range of workshops and presentations on general health promotion.
4.2.3 Tertiary Intervention
Tertiary interventions focus on treating mental health ill health conditions, through psychological/mental health support services.
To comply with this an employee assistance programme was provided. A referral system for occupational health to manage performance and absence, and signposting to specialist mental health services were all put in place.
4.3 The Mental Health Programme
The mental health programme was developed on three themes identified above:
4.3.1 Tackling the stigma around mental health
All sites promoted the National mental health campaigns run by MIND i.e. “time to change”, “time to talk day” and “World Mental Health Day”. Resources were evidence based and available as part of a turn-key package provided by MIND
Mental Health First Aider (MHFA) training was provided by Crossrail so that each of the sites had at least one person to call upon who had a good awareness of mental health issues. The Principal Contractors were also encouraged to offer training to their staff. A job description was developed and volunteers came forward to join the MHFA network. Following initial training, the MHFA network members were invited to regular meetings for on-going training and support, sharing of experiences and peer support. The Crossrail occupational health specialist provided one to one support for the MHFAs post intervention, and a signposting guide was developed. The MHFA network was used to provide individual and team support and awareness.
Storytelling and case studies were encouraged as part of the mental health communication plan. Readily available materials from mental health charities and personal stories from people working on the Crossrail project were used in the regular toolbox talks given on all sites and featured in in-house publications. Senior managers also shared their experience of mental health through Blogs sent to all staff and mental health was one of the key topics used in the Crossrail Health and Safety Impact video series.
4.3.2 Focus on the practical things you can do to help
Crossrail instigated an annual wellbeing programme called Stepping Up Week. Mental health awareness seminars, such as; mental health conditions, stress, fatigue, nutrition, digital detox, exercise and mindfulness, were incorporated into this.
Resilience training was provided for the workforce, focussing on resilient thinking, motivation and engagement and building a personal resilience toolbox i.e. managing personal energy and the impact of technology.
Personal development workshops were available as part of core staff training, including; relationship management, leading teams and time management.
Line manager training on mental health awareness was developed and provision of a line manager’s resource pack was undertaken. The sickness absence-training programme was enhanced to incorporate a case study relating to managing mental health.
Regular displays on mental health topics and information leaflet were provided in racks across all sites. New factsheets were developed i.e. ‘lets talk mental health’, ‘having a difficult conversation’ and ‘sleep’ and were displayed as part of the ‘toilet talker’ series (a single sided leaflet displayed in the toilet area with brief messages on health topics, link to wellbeing and additional support)
4.3.3 Develop solutions by listening
In order to understand the mental health needs on the Crossrail project a staff wellbeing survey was procured, which was validated and allowed for comparison; was quick and easy to use; could be translated into the main languages used on the Crossrail Programme; could be mapped against the HSE Stress Standards [8] ; measured the impact of any interventions and was supported by an organisational psychologist to help with analysis and recommendation for interventions.
Online tools were provided from a number of sources including:- NHS Choices – Live Well[9]
- Mood Juice[10]
- HSE – Work related stress[11]
- Mind Tools[12]
- Sleepio[13]
- Big White Wall[14]
In addition, a number of focus groups were set up. The primary focus group was comprised of the health and safety advisers, wellbeing champions and mental health first aiders. The focus groups were held after the results of the wellbeing survey were made available, in order to understand more about what the results revealed and to allow people to suggest solutions for issues highlighted.
4.4 Launch of the Mental Health Programme
As part of the overall health and safety programme on Crossrail Stepping Up Week is a health and safety engagement initiative held twice per year across all contracts and sites. These events were used to launch the mental health and wellbeing programme. This provided the opportunity to pilot a number of bite-sized initiatives to test out and determine the content of the full Crossrail mental health and wellbeing programme.
The Stepping Up Week Mental Health learning legacy paper details the types of events and initiatives that were implemented. Each site was provided with a range of promotional materials, including; toolbox talks, promotional messages, leaflets, posters and a list of further resources. The Crossrail in-house publications would contain feature articles from across the project.
The initial awareness-raising workshops were soon superseded by resilience and mindfulness workshops incorporated into the full training schedule, with a considerable pull from the workforce for more workshops.
4.5 Measuring Effectiveness
Measuring the effectiveness of the mental health programme focused on both quantitative and qualitative measures such as:
- Crossrail occupational health audit and assurance programme – measuring compliance with mandatory requirements to provide a mental health programme
- Health & Wellbeing Maturity Matrix –with each site committed to improvement in mental health promotion on a yearly basis
- Wellbeing survey – measuring wellbeing improvement year on year and increasing uptake rates
- Interventions – measuring the take up and evaluation of workshops, training and activities
- Review, trending and reporting of occupational health indicators – such as sickness absence data, health surveillance and management referral data.
- Feedback – direct quotes from participants at workshops:
“The best training course I have been on”
“Thank you for an excellent, insightful presentation”
“The toolbox talk on mental health was excellent, you really bought the topic to life in a sensitive and personal way and I know it hit home for a lot of people.”4.5.1 Resilience and Mental Health First Aid Effectiveness
The resilience workshops and mental health first aiders courses were key elements fro increasing staff health and wellbeing focusing on mental health specifically.
Resilience Worshop Effectiveness
The following graphs (in figures 1 and 2) give an indication the results of the satisfaction surveys carried out from the 2 types of resilience workshops held. The course satisfaction was rated on a scale of 1-4 and the results indicate that the courses were very well received.
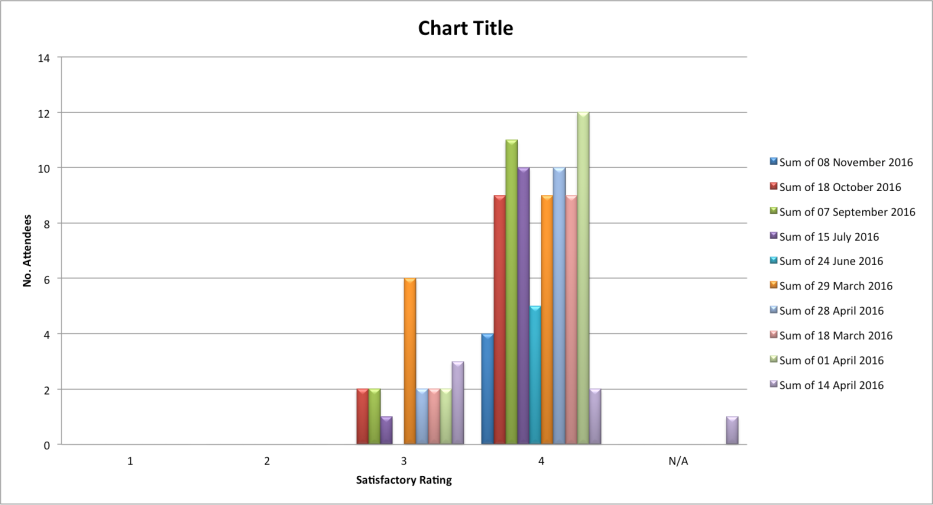
Figure 1 – Satisfaction rating of “Resilience thinking” Course
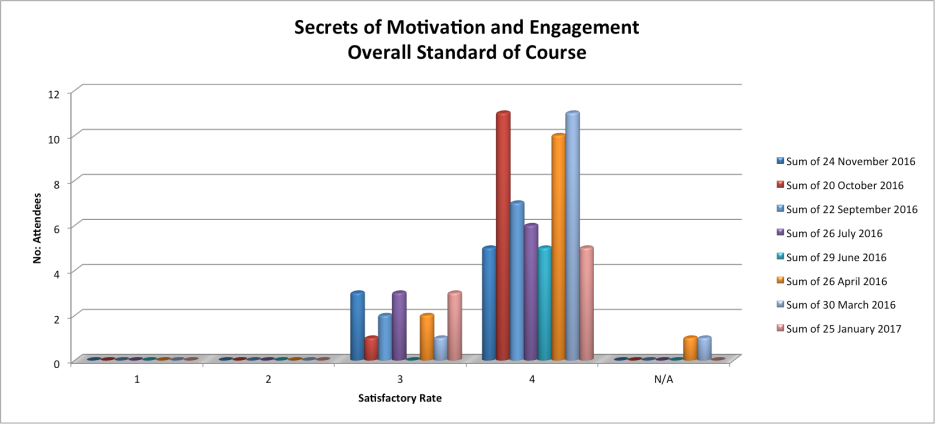
Figure 2– Satisfaction Rating of “Secrets of Motivation and Engagement” Course
Mental Health First Aid Course Effectiveness
There were two different Mental Health First Aid courses run. One was a one day course and the other a two day course. Each was delivered by different providers but, from the feedback obtained, both demonstrated a good transfer of knowledge and delivery of the course. The figures below give an indication of the knowledge levels before and after the courses.
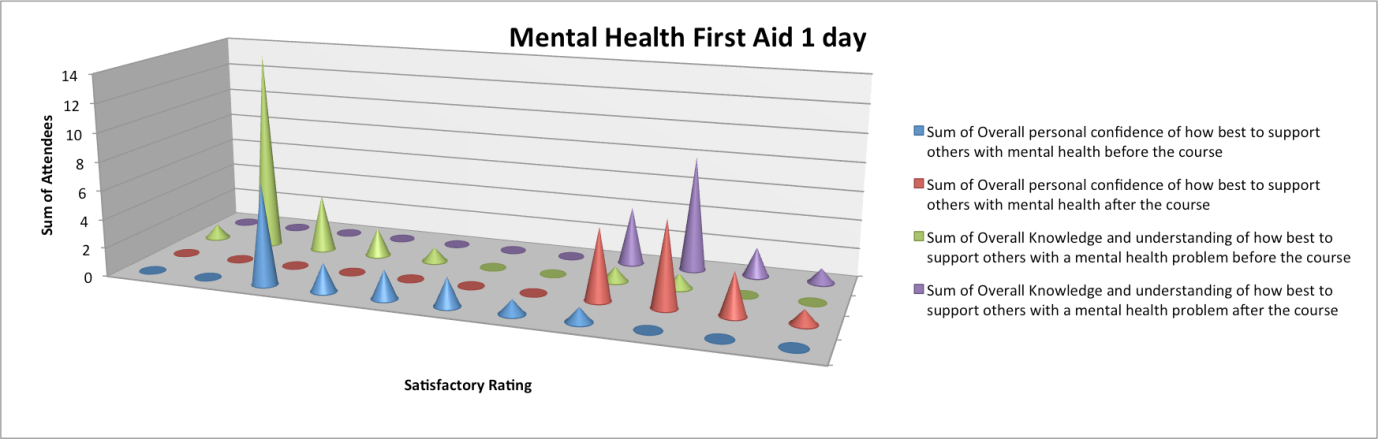
Figure 3 – 1 Day Course – Change in Confidence and Knowledge
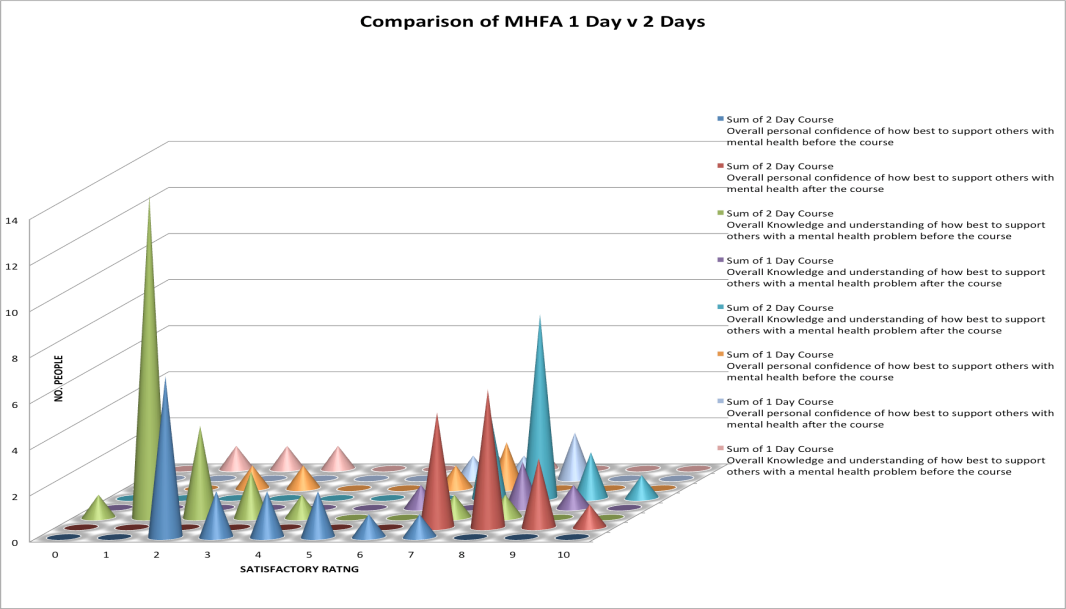
Figure 4 – 2 Day Course – Change in confidence and Knowledge
Assessing the result of the surveys above the outcomes were quantified by the analysis as shown below.
Table 2 – MHFA training outcomes 1 Day Course
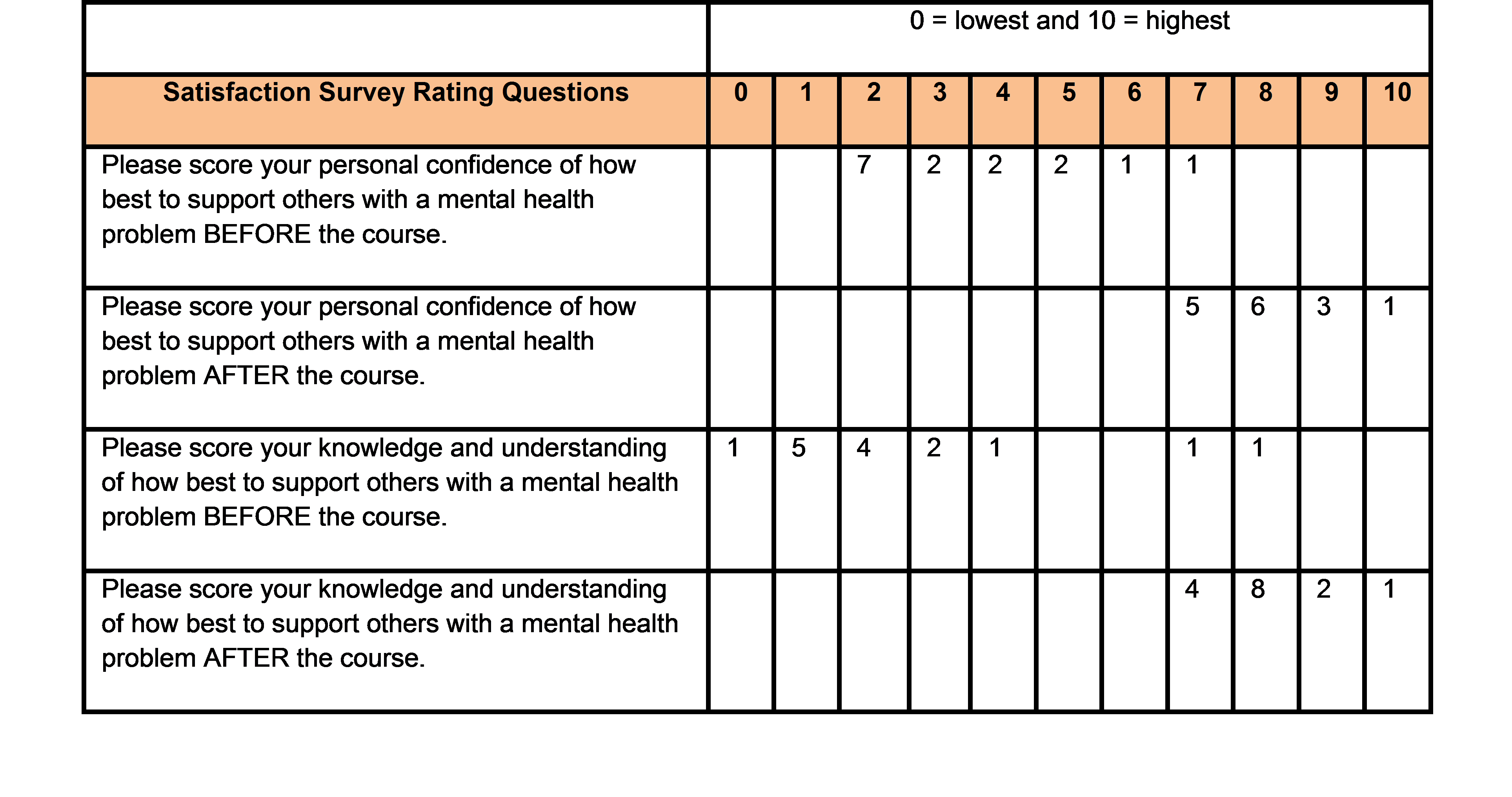
Table 3 – MHFA training outcomes 2 Day Course
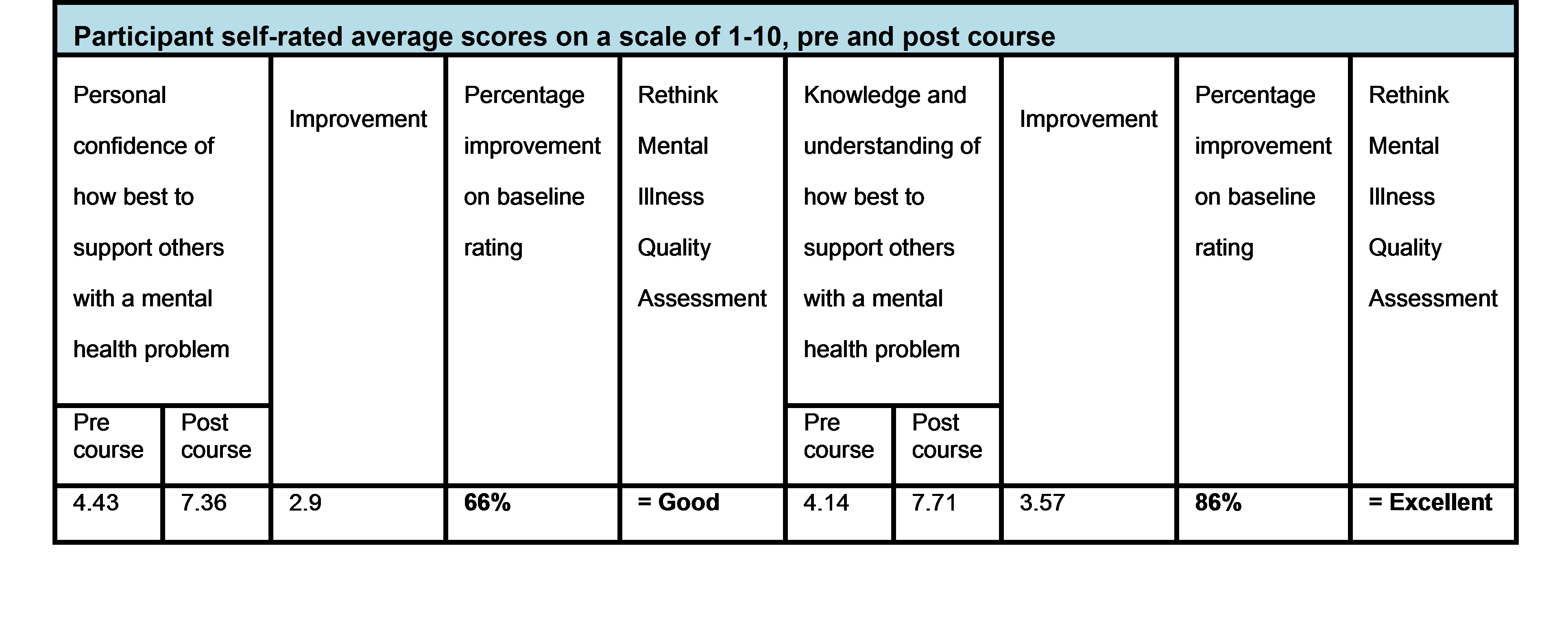
The 2 day course providers quantified the results by percentage. From the responses received personal confidence in dealing with mental health problems increased by 66% and knowledge and understanding of how to support others with mental health problems increased by 88%. This indicates that the training provided good support and increased the knowledge base of the attendees significantly.
The mental health programme continues to develop with the mental health first aiders taking a more active role in promoting good mental health. The resilience workshops are being offered on more sites and the skills are being embedded with follow up workshops. Mental health awareness is part of the annual wellbeing programme and more people are feeling confident about sharing their personal stories.
5.0 Lessons Learned
It is important to take the opportunities created through the greater visibility by campaigns in the media and in the construction industry.
It is vital to tackle any misconceptions about mental health being personal and not something that should be addressed at work.
Professional resources should be made available for managers and staff to help them make informed choices about their heath, and to feel confident to talk about mental health.
Provide the evidence base for senior management. Evaluation of the effectiveness of the courses both quantitative and qualitative is essential.
Normalise mental health by including it in the occupational health and wellbeing strategy and annual improvement plan. Use both qualitative and quantitative measures to demonstrate effective outcomes.
Conduct research into the effectiveness of interventions by external sources and to identify the best way of incorporating a mental health programme that suits the organisation.6.0 Conclusion
Changing the culture of mental health in the workplace can take a long time, depending on how ingrained the present culture is and how committed the leadership team is to embrace a long-term goal.
A range of measurements that are both qualitative and quantitative are required to demonstrate return on investment and the correlation between good mental health and performance.
The benefits and improvements in the workforce health and wellbeing that are achieved will ultimately demonstrate the effectiveness of having this type of programme in place as it will also be demonstrated in the productivity and effectiveness of the organisation.7.0 Recommendations for Future Projects
- The occupational health and wellbeing strategy should include a mental health programme
- The design of any mental health programme should focus on primary, secondary and tertiary intervention
- Consider using the Business in the Community mental health toolkit for employers, which was developed following the national employee mental health survey. The recommendations are:
- Set the tone: we all have mental health
- Address the disconnect
- The role of line manager
- Tackle the culture of silence
- Respond to employees
8.0 References
[1] Health and Safety Executive, Construction Sector statistics. [Online] Available at http://www.hse.gov.uk/statistics/industry/construction/index.htm . Accessed 6 September 2017
[2] Office for National Statistics. (2016) Suicide by occupation, England: 2011 to 2015 article.
[Online] Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/suicidebyoccupation/england2011to2015 [Accessed 21 August 2017][3] Sainsbury Centre for Mental Health. (2009). Briefing 40: Removing Barriers. The facts about mental health and employment. [Online] Available at: http://www.ohrn.nhs.uk/resource/policy/TheFactsaboutMentalHealth.pdf Accessed 6 September 2017
[4] ACAS (February 2016) Promoting positive mental health at work: booklet. Available at: http://www.acas.org.uk/media/pdf/i/o/Promoting_positive_mental_health_at_work(SEPT2014).pdf [Accessed 21 August 2017]
[5] Construction Industry Leadership Group workstream on mental health. [Online], available at: http://www.healthinconstruction.co.uk/ . Accessed 18/9/17
[6] Public Health Responsibility Deal. [Online], available at: https://responsibilitydeal.dh.gov.uk/ Accessed 21 August 2017
[7] London Healthy Workplace Charter. [Online], available at: https://www.london.gov.uk/what-we-do/health/healthy-workplace-charter . Accessed 21 August 2017
[8] HSE Stress Standards. [Online], available at : http://www.hse.gov.uk/stress/standards/. Accessed 21 August 2017
[9] NHS Choices – Live Well, Healthy Living for Everyone. [Online] Available at: http://www.nhs.uk/livewell/Pages/Livewellhub.aspx . Accessed 6 September 2017
[10] Mood Juice. [Online] Available at: http://www.moodjuice.scot.nhs.uk . Accessed 6 September 2017
[11] HSE – Work related stress. [Online] Available at: http://www.hse.gov.uk/stress/dealingwith.htm . Accessed 6 September 2017
[12] Mind Tools. [Online] Available at: https://www.mindtools.com . Accessed 6 September 2017
[13] Sleepio. [Online] Available at: https://www.sleepio.com . Accessed 6 September 2017
[14] Big White Wall. [Online] Available at: http://register.bigwhitewall.com/Eligibility/EligibilityCheck . Accessed 6 September 2017
9.0 Bibliography
The mental health review carried out utilised a number of sources including:
Business in the Community (2016), Mental health at work report: National employee mental wellbeing survey findings. [Online].Available at: https://wellbeing.bitc.org.uk/system/files/research/bitc_mental_health_at_work.pdf Accessed 21 August 2016
HR Review Special Edition, Workplace Wellbeing 2016. [Online] Available at: http://www.hrreview.co.uk/workplace-wellbeing-2016-special-edition .Accessed 21 August 2017
Knapp, M., McDaid, D., & Parsonage, M. (2011). Mental Health Promotion and Mental Illness Prevention: The Economic Case. [Online] Available at: http://gov.uk/government/uploads/system/uploads/attachment_data/file/215626/dh_126386.pdf Accessed 21 August 2017
McManus S, Bebbington P, Jenkins R, Brugha T. (eds.) (2016) Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey 2014. Leeds: NHS Digital. [Online] Available at: http://content.digital.nhs.uk/catalogue/PUB21748/apms-2014-full-rpt.pdf . Accessed 21 August 2017
Mental Health Taskforce to the NHS in England (February 2016), “The five year forward view for mental health”. [Online]. Available at: https://www.england.nhs.uk/wp-content/uploads/2016/02/Mental-Health-Taskforce-FYFV-final.pdf . Accessed 21 August 2017
National Institute for Health and Care Excellence (NICE) (2015) Workplace health: management practices: NICE Guideline [NG13]. [Online] Available at: https://www.nice.org.uk/guidance/ng13 . Accessed August 17
No health without mental health: A cross-government mental health outcomes strategy for people of all ages health, [Online]available at: ww.gov.uk/government/uploads/system/uploads/attachment_data/file/213761/dh_124058.pdf . Accessed August 17
Seymour L. Common mental health problems at work: What we now know about successful interventions. A progress review. London: Sainsburys Centre for Mental Health; 2010.
Waddell G, Burton K (2006) “Is work good for your health and wellbeing?” An independent review. London
-
Authors

Christina Butterworth RN, SCPHN, Hon.FFOM - Crossrail Ltd
Christina is the Crossrail Occupational Health and Wellbeing Specialist, and is ultimately responsible for leading the organisation’s effort to prevent work related ill health and promote good health and wellbeing at work.
Working as part of the Health and Safety Improvement team, she provides high level support and advice on evidence based practice and quality standards. Managing the Crossrail health and wellbeing programme and collaborating with our Principal Contractors on targeted intervention and robust process management.
Christina has had a varied career in occupational health working for a number of large national and international organisations and works tirelessly to continuously improve occupational health and wellbeing. Working with like-minded individuals to provide optimal health for our staff and leadership commitment at all levels.
Christina joined Crossrail in 2014 and works with stakeholders in the Construction and Rail industries to set standards of good practice.